Autonomous Medical AI Agents Are Not Ready to Close the Loop
Nature just published a roadmap toward autonomous medical AI agents. Before we celebrate, let's be precise about what 'autonomous' means when a wrong decision can harm a patient.
The Gap Between a Research Roadmap and a Safe System
A Nature paper published this week lays out a trajectory toward autonomous medical AI agents: systems that perceive clinical data, reason over it, and act without requiring a human to approve every step. The framing is serious and the motivation is real. Clinician burnout, diagnostic delays, and the sheer volume of routine decisions that flood health systems every day represent a genuine problem that better automation could help solve.
But there is a precise engineering problem buried inside that optimistic framing, and it is worth being direct about it: closing the loop autonomously in a clinical context is a different class of problem from closing the loop in a warehouse or a recommendation feed. The consequences of a wrong action are not reversible with a retry. The regulatory surface is enormous. And the observability requirements for autonomous operation in regulated health contexts are not yet well-defined in practice, even as the EU AI Act guidelines and FDA SaMD frameworks are actively being drafted.
This is not an argument against progress. It is an argument for precision about where the hard problems live.
What Autonomy Actually Means in Control Systems Terms
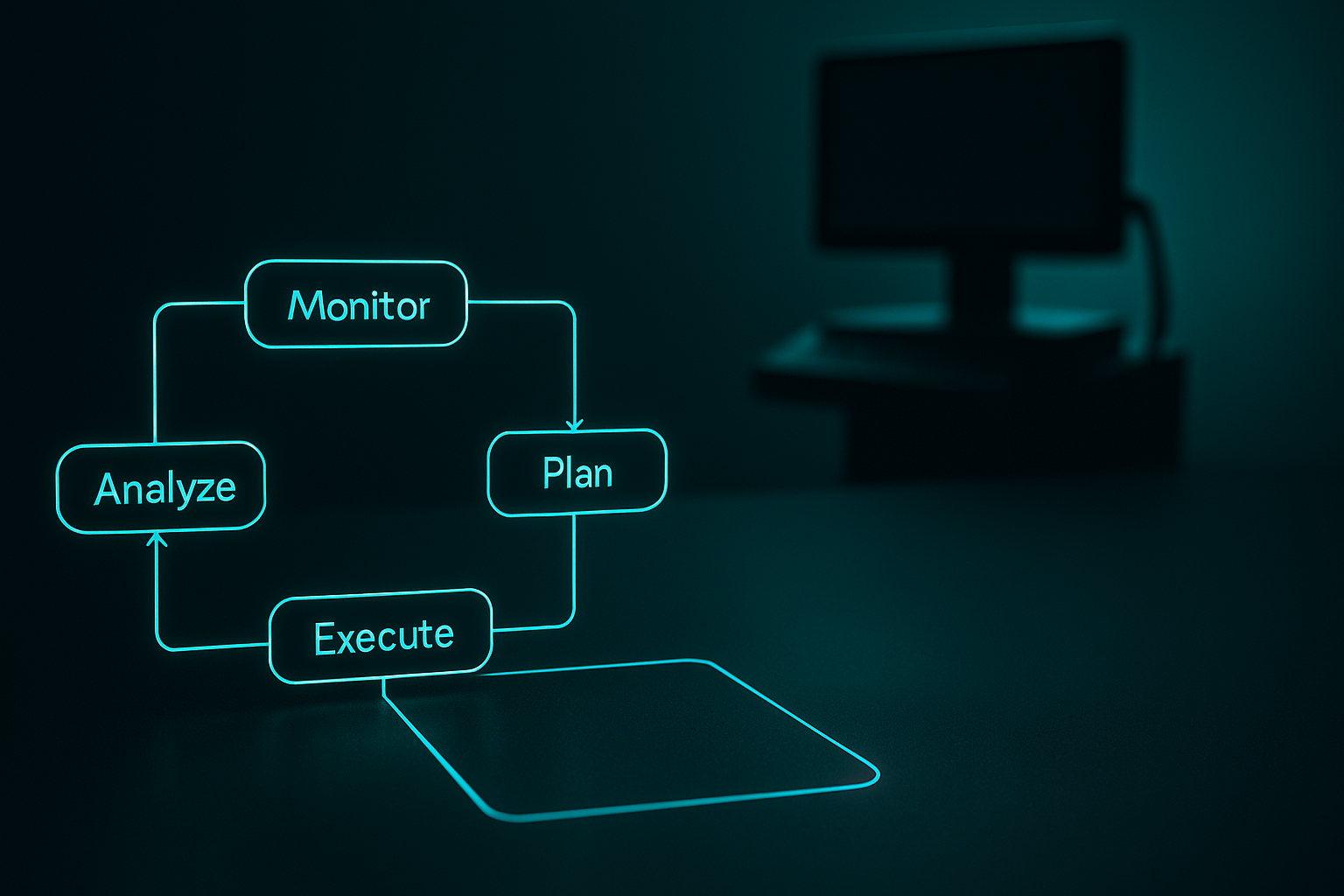
In autonomous systems engineering, the standard framing is the MAPE-K loop: Monitor, Analyze, Plan, Execute, with a shared Knowledge base underpinning all four phases. The question of autonomy is not binary. It lives on a spectrum defined by which phases have human checkpoints and at what latency.
In most clinical AI deployments today, the loop is deliberately broken at the Execute phase. A model might monitor vitals, analyze deterioration risk, and generate a care plan suggestion, but a nurse or physician approves the action before it propagates into the EHR or triggers a medication change. This is sometimes called human-in-the-loop design, but from a control systems perspective it is more precise to call it supervised autonomy with gated execution.
The Nature roadmap and the broader push toward autonomous medical agents proposes moving the human checkpoint upstream, or removing it from the critical path entirely for lower-risk decisions. The architectural implication is significant: the Knowledge base must now carry not just clinical heuristics but also confidence thresholds, escalation triggers, fallback policies, and audit trails that satisfy post-market surveillance requirements.
Building that knowledge base correctly is harder than building the model.
Where the Engineering Complexity Concentrates
Confidence calibration under distribution shift. A clinical AI agent making autonomous decisions must know when its own model is operating outside the training distribution. In a hospital context, distribution shift is not a rare edge case. It happens when patient demographics change, when a new protocol is introduced, when an EHR vendor updates a data schema, or when seasonal disease patterns shift. Monitoring for drift in a supervised setting is already non-trivial. Monitoring for it in a closed-loop autonomous system, where the agent's own actions may alter the data distribution it subsequently observes, is a feedback problem that requires explicit architectural design, not just an anomaly detection sidecar.
Accountability chains under the EU AI Act. The Commission's draft guidelines for classifying high-risk AI systems make clear that clinical decision support tools that influence patient management are likely to sit in the high-risk category. For those systems, the Act requires risk management documentation, logging sufficient for post-market surveillance, and meaningful human oversight. "Meaningful oversight" is the phrase that matters. If an autonomous agent executes 200 micro-decisions per shift and a human reviews a summary dashboard once per hour, it is not obvious that this satisfies the oversight requirement. The legal interpretation is still being worked out, and engineers building these systems need to make conservative architectural assumptions right now.
The pilot overload problem. Modern Healthcare flagged this week what practitioners inside health systems already know: hospitals are running too many AI pilots simultaneously, with insufficient infrastructure to evaluate them rigorously or retire them when they underperform. Autonomous agents amplify this problem because a poorly performing supervised tool produces bad recommendations that a clinician can ignore, while a poorly performing autonomous tool produces bad actions that propagate into care delivery before anyone notices. The operational maturity required to run autonomous AI safely is higher, not lower, than what most health systems currently have.
Trust as a load-bearing infrastructure component. Healthcare IT News framed trust as infrastructure this week, and that framing resonates technically. In a distributed system, trust is operationalized through cryptographic proofs, audit logs, access controls, and monitoring. In a clinical AI system, trust also requires that every stakeholder, including the patient, can query the system about why a particular decision was made and receive a legible answer. Explainability is not a nice-to-have in this context. It is a prerequisite for the accountability chain that regulation requires and that clinical governance demands.
What a Safer Architecture Actually Looks Like
If the goal is to move toward more autonomous, responsible operation, the architecture needs to solve several problems simultaneously.
First, the Monitor phase needs to be separated from the model itself. An independent observability layer, ideally one that does not share weights or preprocessing pipelines with the decision model, should continuously evaluate input distribution, output confidence, and downstream outcome correlations. When that monitor detects anomaly, it should route to human review, not to the Execute phase.
Second, the Knowledge base needs explicit policy encoding. Not implicit policy learned from training data, but explicit, version-controlled rules that define when the agent is permitted to act, when it must escalate, and what constitutes a safe fallback. This is closer to formal methods than to machine learning, and it requires clinical governance participation to write correctly.
Third, the Execute phase should implement graduated autonomy by action risk tier. Scheduling a follow-up appointment autonomously carries different stakes than adjusting a medication dose. The architecture should enforce that higher-risk actions have shorter human-review windows and lower confidence thresholds for escalation, not treat all outputs from the model as equivalent.
Fourth, post-market surveillance needs to be designed into the system from the start, not bolted on. Every autonomous action should generate a structured audit event that maps to the regulatory reporting schema your jurisdiction requires. Building this retroactively is expensive and usually incomplete.
What the Research Community and Industry Need to Converge On
The Nature roadmap is valuable because it names the destination clearly. What the field now needs is equivalent precision about the intermediate states and the failure modes at each transition.
Specifically: what is the minimum viable observability infrastructure for a clinical AI agent to be considered safely autonomous at a given risk tier? What does a standardized audit event schema for autonomous clinical actions look like, and can it be shared across EHR vendors? How should confidence thresholds be set and validated for pediatric populations, where training data is structurally sparse and distribution shift is pronounced as children grow?
These are engineering and regulatory questions, not research questions. Answering them requires close collaboration between system builders, clinical informaticists, and regulators before autonomous agents are widely deployed, not after the first serious adverse event.
The hospital AI story that The Atlantic covered this week is real: AI is already inside hospitals, running in more clinical workflows than most patients realize. The question is not whether autonomous agents will arrive. It is whether the control infrastructure will be ready when they do.
Takeaway for Practitioners
If you are building or evaluating clinical AI systems, three concrete actions matter right now.
One: map every inference your system makes to a point on the autonomy spectrum and identify the human checkpoint at each point. If checkpoints are missing for high-risk actions, treat that as a critical architectural defect, not a future roadmap item.
Two: start building your audit event schema against the EU AI Act high-risk requirements today, even if you are not yet in a jurisdiction where it applies. The FDA's SaMD post-market surveillance expectations are converging toward similar requirements. Designing to the stricter standard now costs less than migrating later.
Three: treat distribution shift monitoring as a first-class system component. Budget engineering time for it proportional to the stakes of autonomous action, not proportional to how difficult it is to sell to a product roadmap committee.